

What Is NAD and What Does the Evidence Actually Say?
Originally published September 2025. Updated February 2026.
NAD⁺ is everywhere right now, marketed as a shortcut to “more energy,” “cellular repair,” and “anti-aging,” often through NAD⁺ infusions or NAD⁺ shots.
But NAD⁺ biology is real science, not a slogan. And the clinical evidence is more nuanced than most marketing suggests.
Research Update: What’s New in 2026?
In our PRISMA-guided systematic review published in Ageing Research Reviews, we evaluated NAD⁺-related interventions for anti-aging and wellness outcomes across both human and rodent intervention studies (January 2010–October 2025).
In plain language: we mapped the current evidence so we can talk about NAD⁺ with precision instead of assumptions, especially as marketing for NAD⁺ IV therapy, NAD⁺ injections, and “NAD⁺ shots” has gotten louder than the data.
Quick Takeaways
- Oral NAD⁺ “precursors” (like NR and NMN) reliably raise NAD⁺-related biomarkers in human studies (biochemical “target engagement”).
- But improvements in outcomes people care about—energy, metabolic health, vascular health, physical performance—are mixed and often endpoint-specific.
- Despite widespread marketing of NAD⁺ IV drips and NAD⁺ shots, we found no eligible outcomes trials evaluating IV or IM NAD⁺ itself for anti-aging or wellness indications. These methods also face biological limitations: NAD⁺ is not expected to freely enter cells intact and is typically broken down outside the cell, meaning “direct cellular refill” is an oversimplification of how NAD⁺ biology actually works.
What Is NAD?
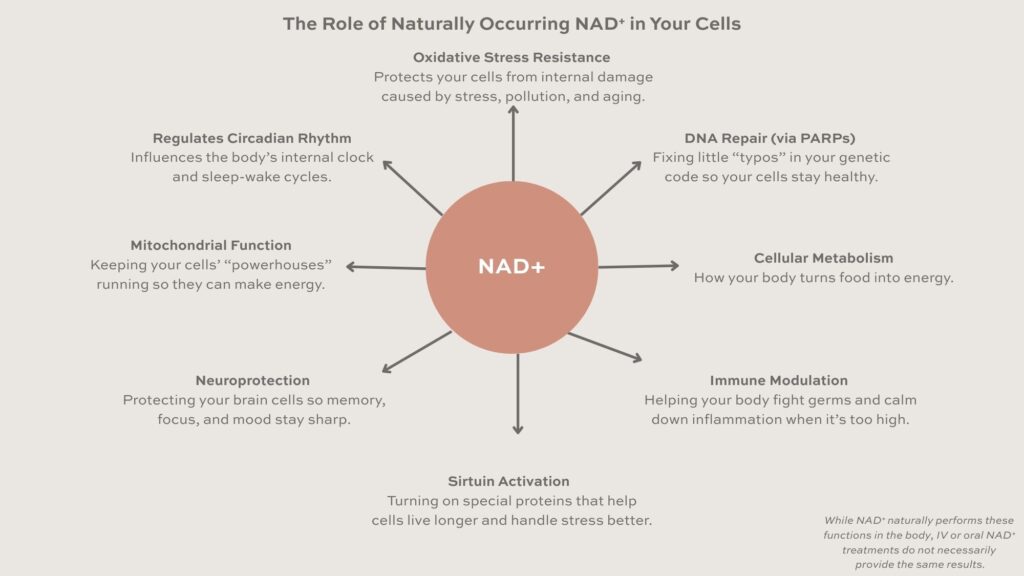
NAD stands for nicotinamide adenine dinucleotide. It’s a molecule your cells use constantly. It plays central roles in:
- Energy metabolism (helping convert nutrients into usable cellular energy)
- Redox balance (NAD⁺ and NADH shift back and forth as part of metabolism)
- Cellular maintenance pathways often discussed in aging biology
You’ll see two forms referenced most often:
- NAD⁺ (oxidized form)
- NADH (reduced form)
Most “longevity” conversations focus on NAD⁺ because it’s involved in pathways tied to cellular maintenance and stress responses.
Why Is NAD⁺ Linked to Aging and Wellness?
Aging biology is complex, but NAD⁺ metabolism appears to change with age. Researchers have reported lower NAD⁺ availability in certain tissues and age-associated conditions, though the size and consistency of decline can vary depending on tissue and how NAD is measured.
This is why “NAD⁺ boosting” strategies exist: if NAD⁺ biology shifts with age, restoring NAD⁺-related pathways might support aspects of healthspan.
The key word is might – because biology is not the same as outcomes.
NAD⁺ Supplements vs. NAD⁺ Infusions vs. NAD⁺ Shots: What’s the Difference?
This is where a lot of online content collapses important distinctions.
NAD⁺ precursors (supplements)
Most human research has focused on oral “precursors”, ingredients your body can use to build NAD⁺ through established pathways. The most common:
- Nicotinamide riboside (NR)
- Nicotinamide mononucleotide (NMN)
- Nicotinamide (NAM / niacinamide)
- Niacin (nicotinic acid)
Across human trials, NR and NMN most consistently show increases in NAD⁺-related metabolites in blood-derived measures. That’s the strongest and most consistent signal in humans: supplementation can shift measurable NAD⁺-related biochemistry.
NAD⁺ IV therapy / NAD⁺ infusions
NAD⁺ IV therapy means infusing NAD⁺ itself into the bloodstream. It’s commonly marketed as:
- faster
- more bioavailable
- more powerful than supplements
- “directly replenishing cellular NAD⁺”
Those are strong claims. The problem is that “sounds plausible” is not the same thing as “biologically validated,” and the most popular mechanism used to sell it is oversimplified (more on that below).
In the anti-aging/wellness context, outcomes-quality clinical evidence for IV NAD⁺ remains a major gap relative to how confidently it is marketed.
NAD⁺ injections / NAD⁺ shots
“NAD⁺ shots” usually mean intramuscular (IM) or subcutaneous (SubQ) NAD⁺ injections.
The evidence issue is similar, because these shots still work their way through the bloodstream and face the same biological limitations.
A Necessary Caveat: Biological Plausibility (and why marketing often gets it wrong)
Even before you get to clinical outcomes, it’s worth addressing the most common claim used to sell NAD⁺ infusions and NAD⁺ shots:
“This is better because you’re directly replenishing NAD⁺.”
That’s an oversimplification.
NAD⁺ is a large, highly polar dinucleotide. In general, molecules with those properties do not freely cross mammalian cell membranes in intact form. So the idea that IV or IM NAD⁺ simply enters cells and “refills” intracellular NAD+ directly is not a given.
What is more biologically plausible is that extracellular NAD⁺ is processed by enzymes outside the cell into smaller metabolites (for example, nicotinamide and related breakdown products). Those smaller components can then be taken up and used through intracellular salvage pathways that rebuild NAD⁺ inside the cell. This is what appears to have taken place during the only published pilot study of IV NAD⁺ infusions.
In other words: even if IV/IM NAD⁺ influences intracellular NAD biology, the most plausible mechanism is often indirect, through breakdown and recycling in a manner similar to taking precursors in the first place, rather than “NAD⁺ goes straight into your cells intact.”
How to Interpret The Evidence: Biomarkers vs Outcomes
This matters because it’s a reminder to separate two questions:
- Can we change NAD-related biomarkers? (often yes with certain approaches)
- Do we reliably improve meaningful outcomes in humans, safely and durably? (still mixed and not settled)
When a therapy is marketed with a mechanism that is oversimplified, it becomes even more important to demand strong outcomes evidence.
What benefits are actually supported in humans?
This is where nuance matters. NAD biology is real. But “real biology” doesn’t automatically equal consistent real-world benefits.
Biomarkers: often yes
Many human trials show that oral NR and NMN can raise NAD-related metabolites in blood-derived measures. This is consistent and repeatable.
However, tissue-level effects can be more variable, and “biomarker moved” does not automatically mean “you will feel different” or “aging is reversed.”
Energy, fatigue, performance: mixed
Trials have evaluated physical performance and functional outcomes in different ways – VO2max/peak, grip strength, submaximal performance tests, walking tests, fatigue scales, and more.
A common pattern is heterogeneity: some endpoints move, many do not, and effects (when present) may be more likely to appear in certain functional or submaximal measures than in headline metrics like VO2max or grip strength.
Metabolic markers and body composition: mixed
Metabolic endpoints show up frequently: insulin sensitivity, glucose measures, lipids, hepatic fat, and inflammatory markers.
Across the human evidence base, results vary by endpoint and population. Some trials report improvements in specific measures; other well-controlled trials show no meaningful difference versus placebo for commonly marketed claims—despite biomarker changes.
Vascular markers: mixed
Blood pressure and arterial stiffness have been evaluated in a smaller subset of trials, with variable results across endpoints and populations.
Skin/aesthetic outcomes: rarely studied in humans
If you’re seeing strong marketing claims that NAD⁺ infusions or NAD⁺ injections meaningfully improve visible aging or aesthetic outcomes, it’s important to understand that these specific outcomes are not heavily represented in outcomes-quality human trials.
Why Do Rodent Studies Often Look More Impressive?
Rodent intervention studies are often more uniformly positive across metabolic, mitochondrial, inflammatory, and functional measures. This supports biologic plausibility for NAD⁺-linked pathways.
But translation from rodent models to human aging is never automatic. Differences in physiology, timing, dosing exposure, endpoints, and the complexity of human aging all contribute to the common pattern we see in longevity science:
Strong animal signal, but mixed human outcomes.
Are NAD IV Therapies or Shots FDA-Approved?
NAD⁺ infusions and NAD⁺ injections are not FDA-approved treatments for anti-aging or wellness outcomes, and there are no universally accepted clinical guidelines defining standardized dosing, long-term safety, or validated endpoints for “wellness NAD⁺ therapy.”
Dietary supplements (NR/NMN/NAM/niacin) are also not FDA-approved to treat or prevent disease.

Side effects and risks: what we can say responsibly
Across randomized trials, oral NAD⁺-precursor interventions are generally reported as well tolerated over weeks to months, with no consistent serious safety signals over the durations studied.
For parenteral approaches (IV/IM/SubQ), the issue is not that we can claim definitive harm in wellness contexts. The issue is that marketing confidence exceeds the long-term outcomes-quality evidence base and the most common mechanistic explanation used to sell NAD IV therapy is oversimplified. Unless further studies show a unique benefit, it currently appears to be a more expensive, riskier, and less convenient method of supplementation relative to oral precursors.
How to think about NAD without getting pulled into hype
If you’re trying to make sense of NAD supplements versus NAD⁺ injections versus NAD⁺ infusions, here’s the most honest frame:
- NAD augmentation can be biologically active (biomarker shifts are real).
- Human clinical effectiveness for anti-aging/wellness outcomes remains inconclusive (mixed and endpoint-specific).
-
For NAD IV therapy and NAD shots specifically, the typical “direct cellular refill” explanation is oversimplified; the biologically plausible story is breakdown and salvage, and it does not currently have evidence of any unique benefit over oral precursor supplementation.
Frequently Asked Questions
What is NAD?
NAD (nicotinamide adenine dinucleotide) is a coenzyme found in every cell. It supports energy metabolism, redox balance, and cellular maintenance pathways often discussed in aging biology.
What’s the difference between NAD⁺ and NADH?
NAD⁺ is the oxidized form and NADH is the reduced form. They convert back and forth during normal metabolism as cells move electrons to generate energy.
What are NAD infusions (NAD IV therapy)?
NAD infusions deliver NAD⁺ intravenously and are often marketed as a way to “directly replenish cellular NAD.” The more biologically plausible story is indirect: NAD⁺ is not expected to freely enter cells intact and is typically broken down outside the cell into smaller metabolites that can be salvaged to rebuild intracellular NAD.
What are NAD shots (NAD injections)?
“NAD shots” usually refer to intramuscular (IM) or subcutaneous (SubQ) injections of NAD⁺. While they’re often promoted as faster or more “direct,” they still enter systemic circulation and face the same biological limitation: NAD⁺ is unlikely to simply pass into cells intact, so any effect is more plausibly mediated through breakdown and salvage.
Are NAD shots the same as NAD IV infusions?
No. NAD shots are typically IM or SubQ injections, while NAD IV infusions deliver NAD⁺ through a vein. These routes aren’t interchangeable, and neither automatically implies better cellular uptake.
Why is “direct cellular NAD refill” considered biologically implausible?
Because NAD⁺ is a large, highly polar dinucleotide and is not expected to freely cross mammalian cell membranes intact. Outside the cell, NAD⁺ is typically processed into smaller metabolites (such as nicotinamide), which can then be taken up and used through salvage pathways to rebuild NAD inside the cell.
Do NAD infusions help with energy?
Some people report feeling better after an infusion, but subjective experiences don’t equal proven, durable clinical effects. Any perceived benefit may relate to hydration, placebo effects, or short-lived biochemical changes rather than a sustained “cellular reset.”
Do NAD infusions or NAD shots work faster than oral NAD precursors?
Not necessarily. Injected or infused NAD⁺ can be rapidly broken down in the bloodstream, after which components may be salvaged, conceptually similar to how oral precursors support NAD through established pathways. Oral precursors have also been shown to raise NAD-related metabolites within hours, so “faster” is not a guarantee.
Are NAD infusions or NAD shots FDA-approved for anti-aging or wellness?
No. NAD infusions and NAD injections are not FDA-approved treatments for anti-aging or wellness outcomes, and there are no universally accepted clinical guidelines defining standardized dosing, validated endpoints, or long-term safety for “wellness NAD therapy.”
What’s better: NR or NMN?
Both NR and NMN have human evidence showing increases in NAD-related biomarkers, but outcomes are mixed and context-dependent. The better choice depends on the goal, dose, duration, product quality, and individual health context, none of which has a universal answer today.
Reference
Gallagher, Cory; Emmanuel, Owoturo Oluwaseun. NAD⁺ supplementation for anti-aging and wellness: a PRISMA-guided systematic review of preclinical and clinical evidence. Ageing Research Reviews. 2026;103057. https://doi.org/10.1016/j.arr.2026.103057
